The Truth About Fluoride
For decades, fluoride has been promoted as a cornerstone of dental health, but its history tells a very different story. Long before it found its way into toothpaste and tap water, fluoride was an industrial byproduct tied to lawsuits, secrecy and powerful public relations campaigns. Today, new research challenges the narrative that fluoridation is a safe and essential public health measure, raising serious questions about its risks, ethics and effectiveness.
A Hidden History
Fluoride’s story begins not in dentistry but in heavy industry. By the 1930s, the Aluminum Company of America (Alcoa) faced lawsuits from farmers and workers poisoned by fluoride emissions (Bryson, 2004). When the Manhattan Project required vast amounts of fluoride to enrich uranium for atomic weapons, secrecy and liability converged. Harold Hodge, the project’s chief toxicologist, pivoted fluoride from toxic threat into supposed dental benefit, embedding it into U.S. health policy (Griffiths & Bryson, 1997).
The 1945 Newburgh–Kingston fluoridation “trial,” publicly marketed as a dental health study, was in fact monitored by atomic scientists collecting blood samples for classified research (Griffiths & Bryson, 1997). What began as an industrial liability management scheme evolved into one of the most enduring public health policies of the 20th century.
Manufacturing Consent
The fluoridation campaign was driven less by science than by public relations. Edward Bernays, the “father of PR,” applied the same tactics he used to sell cigarettes to women, reframing industrial waste as medicine (Bernays, 1928/2005).
Critics who raised concerns were discredited. Dr. Phyllis Mullenix, a toxicologist at the Forsyth Dental Center, lost her position after publishing evidence that fluoride was neurotoxic in animals (Mullenix et al., 1995). The message was clear: challenging the fluoride orthodoxy carried professional risk.
Questioning the Science
While fluoride undeniably interacts with enamel, the picture is not as clear as its promoters suggest:
- Topical vs systemic effects: The only proven benefit of fluoride is topical, not systemic. Swallowing it confers no advantage and only increases toxic exposure (Iheozor-Ejiofor et al., 2015).
- Fluorapatite vs hydroxyapatite: Fluoride incorporation into enamel converts natural hydroxyapatite into fluorapatite. While fluorapatite is harder and more acid-resistant, it is also more brittle, making teeth less resilient to functional stress (Featherstone, 1999; Elliott, 1994). This undermines the very premise of fluoridation, since the “strengthening” may actually compromise tooth integrity.
- Neurotoxicity: Over fifty human studies now link fluoride exposure to lowered IQ in children. A 2019 JAMA Pediatrics study found prenatal exposure associated with measurable reductions in cognitive performance at levels typical of U.S. water supplies (Green et al., 2019).
- Endocrine disruption: Fluoride interferes with thyroid function and inhibits critical enzymes — a property once exploited by the Manhattan Project to detect nuclear contamination (National Research Council, 2006).
A Global Outlier
Ninety-seven percent of Western Europe has rejected water fluoridation. Countries such as Germany, Sweden, and the Netherlands rely instead on topical fluoride or alternative caries prevention strategies, yet their dental health equals or surpasses that of fluoridated nations (Cheng, Chalmers, & Sheldon, 2007).
Nobel laureate Arvid Carlsson, who advised Sweden’s government, argued that even if fluoride had a benefit, mass medication without consent violated medical ethics (Carlsson, 1978).
The Industrial Loophole
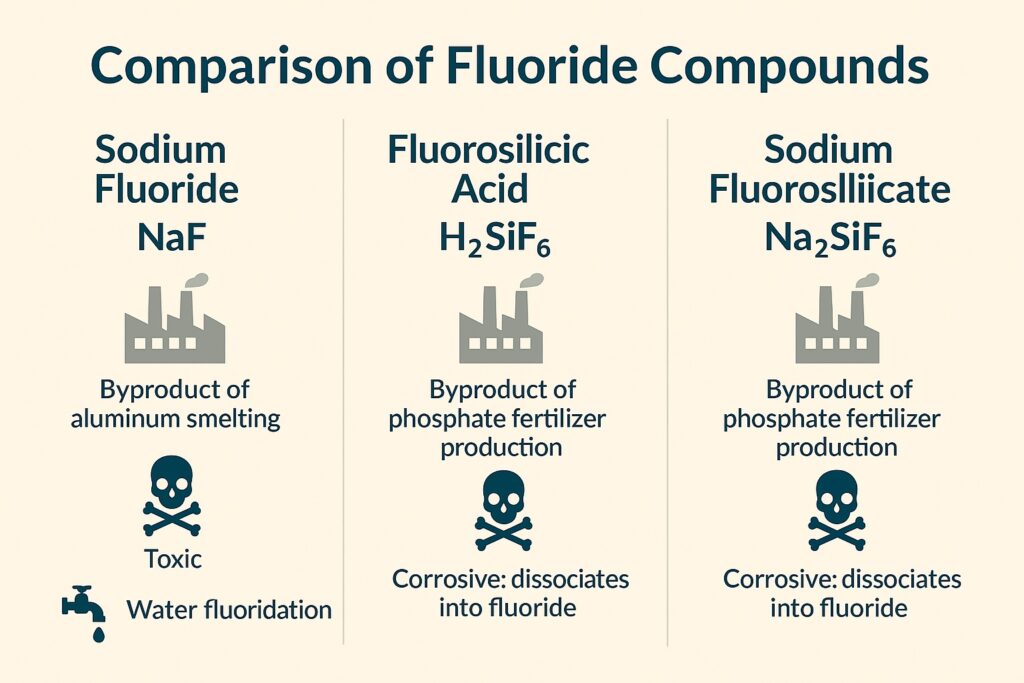
Today, more than 90% of fluoridated U.S. water is treated not with pharmaceutical-grade sodium fluoride but with fluorosilicic acid — hazardous waste collected from phosphate fertilizer smokestacks (Coplan et al., 2007).
This substance contains arsenic, lead, and radionuclides. It would be illegal to discharge into rivers, yet when rebranded as a “water treatment chemical,” it becomes a profitable disposal pathway for industry.


Why Fluoridation Remains Entrenched
1. Historical Legitimacy and Loss of Face
Fluoridation was introduced as a symbol of scientific progress. To admit error now would be to acknowledge that generations of dentists and public health officials misled the public. The American Dental Association (ADA) continues to defend fluoridation as a pillar of its identity (American Dental Association, 2018).
2. Industrial and Political Alliances
Fluoridation aligned public health policy with industrial waste disposal, benefiting phosphate fertilizer and aluminum producers. These industries maintain lobbying influence. Regulatory bodies like the CDC and EPA have been criticized for regulatory capture, prioritizing defense of policy over emerging evidence (NRC, 2006).
3. Scientific Entrenchment and Misinformation
- Much of the pro-fluoridation evidence dates to the mid-20th century. Modern reviews find weak or no systemic benefit (Iheozor-Ejiofor et al., 2015).
- Dissenting scientists, such as Mullenix, were marginalized (Mullenix et al., 1995).
- Defenders shift arguments, claiming fluoridation is essential for reducing health disparities, despite international evidence to the contrary (Cheng et al., 2007).
4. Indoctrination in Dental Education
Fluoride is taught as dogma in U.S. dental schools. Students are rarely exposed to modern critiques and risk being stigmatized as “anti-science” if they dissent (Connett, Beck, & Micklem, 2010). This ensures new generations of dentists inherit old talking points.
5. Legal and Financial Fallout
Recognizing harm from fluoridation would open municipalities, associations, and industry to massive liability. The fluoride-based dental product market — varnishes, rinses, toothpaste — represents billions in revenue (Griffiths & Bryson, 1997).
6. The Politics of Admitting Harm
Fluoride has become a proxy for public health authority. If fluoridation is discredited, it risks undermining trust in other mass interventions. For this reason, critics are often painted as fringe voices, regardless of their credentials (Connett et al., 2010).
Conclusion
The fluoride story is not one of science serving the public, but of industry and institutions protecting themselves. Even its supposed benefit — forming fluorapatite — comes with a hidden cost of brittleness that may compromise enamel resilience. The convergence of evidence now suggests a simple truth: fluoride is not necessary for dental health, ingestion carries systemic risks, and water fluoridation represents one of the most audacious public health deceptions of the 20th century — a deception that remains politically defended to this day.

Dr. Gerry Curatola
Dr. Gerry Curatola is a renowned biologic restorative dentist with more than 40 years of clinical practice experience. He studied neuroscience at Colgate University and attended dental school at the New York University (NYU) College of Dentistry where he now serves as Adjunct Clinical Associate Professor in the Department of Cariology and Comprehensive Care.
Dr. Gerry Curatola
Dr. Gerry Curatola is a renowned biologic restorative dentist with more than 40 years of clinical practice experience. He studied neuroscience at Colgate University and attended dental school at the New York University (NYU) College of Dentistry where he now serves as Adjunct Clinical Associate Professor in the Department of Cariology and Comprehensive Care.